Keeping clinical documentation compliant and accurate is a challenge we all face in healthcare. It’s not just about avoiding penalties—it’s about creating reliable patient records that truly reflect the care we provide.
Here are some key practices to help ensure your documentation meets compliance standards while also being thorough and precise.
Why Compliance Matters in CAPD
Compliance in clinical documentation is crucial for many reasons. Beyond avoiding penalties, it ensures that patient records are accurate and comprehensive, which is essential for quality care and operational efficiency. Poor documentation can lead to denied claims, financial losses, and even compromised patient care.
Key Practices for Effective and Compliant Documentation
- Documenting Every Query: Every query should be documented to demonstrate compliance and validate the need for the query. This creates a clear audit trail and ensures all regulatory requirements are met.
- Keeping Query Titles Neutral: Make sure your query titles are neutral and objective. They should not suggest a purpose beyond clarifying information, maintaining the integrity of the documentation process.
- Following Established Guidelines: Stick to the “Guidelines for Achieving a Compliant Query Practice (2019 Update).” Queries should be designed to avoid leading the provider to a specific answer, supporting unbiased and accurate documentation.
- Including Relevant Clinical Indicators: Every query should reference relevant clinical indicators from the patient’s health record. This makes the queries specific and contextually appropriate, which supports thorough documentation.
- Avoiding Undocumented Diagnoses: Ensure that queries do not suggest diagnoses that are not documented in the patient’s record. This helps maintain the objectivity of the documentation process and the provider’s clinical judgment.
- Offering Reasonable Choices: The options provided in queries should reflect reasonable conclusions based on the patient’s situation. This keeps the documentation logical and patient-focused.
- Using Prior Information Carefully: Prior health records should be used only if they are relevant to the current encounter and comply with facility policies. For inpatient records, stick to the current inpatient data to maintain integrity.
- Linking to Clinical Indicators: Providing links within the health record to access clinical indicators can enhance the usability of queries and help providers make informed decisions.
- Excluding Financial Impact from Queries: Avoid mentioning the impact on reimbursement, payment methods, quality metrics, or severity of illness in the query process. This keeps the focus solely on clinical accuracy and necessity.
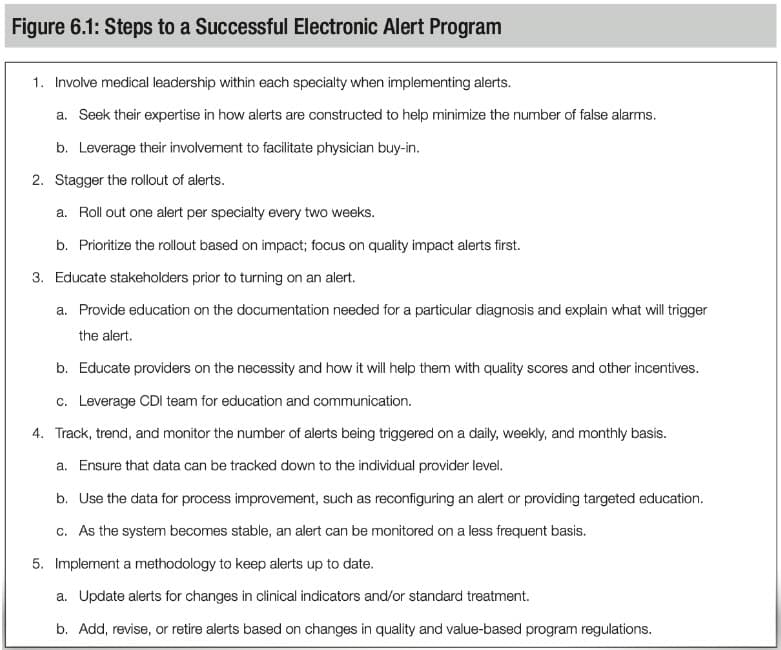
Note, it is also important to consider alert fatigue. “Because of the increasing number of alerts facing the provider,” states Karen Newhouser, RN, BSN, CCDS, CCDS-O, CCS, CDIP, CCM in ACDIS’ The Provider Query Toolkit: A Guide to Compliant Practices, “ it is important to be careful not to create too many documentation alerts to avoid adding to alert fatigue once the alerts begin to be sent directly to the provider. Being proactive allows for a positive outcome down the road.”
Leveraging Technology for Better Documentation
Technology can greatly assist in maintaining compliance and enhancing clinical documentation. Advanced Clinical Documentation Improvement (CDI) and Clinical Decision Support (CDS) systems can integrate into existing workflows, reducing administrative burdens and improving the quality of care. These systems support real-time decision-making and documentation, ensuring every query is compliant and relevant.
The Power of AI and Machine Learning
Artificial Intelligence (AI) and Machine Learning (ML) are revolutionizing CDI and compliance practices. AI-driven systems can analyze vast amounts of data to identify patterns and suggest improvements in real-time. This technology not only ensures compliance but also improves the accuracy and efficiency of documentation, leading to better patient outcomes.
Final Thoughts
Ensuring compliance in clinical documentation is an ongoing process that requires diligence, detail, and the right technological support. By adopting best practices and leveraging advanced CDI and CDS systems, we can ensure our documentation is accurate, compliant, and of the highest quality, ultimately leading to better patient care and smoother operations.
For more insights on improving clinical documentation and compliance, get in touch with our team to get a demonstration of Epic/HITEKS solution. Epic (powered by HITEKS) has the leading physician-facing CAPD tool for CDI and surpasses compliance requirements for CAPD.